.
.
. 2011.
This case reviews the policy changes in tobacco control in post-apartheid South Africa from 1994 to 1996 under the leadership of Minister of Health Dr. Nkosazana Zuma. After providing contextual information on South Africa, including historical, demographic, social, and health information, the case delves into the history of tobacco and of global tobacco control efforts. The case then details the history of tobacco in South Africa, including data collection, epidemiology, early control efforts, and the policy efforts of the mid-1990s. The case describes the African National Congress (ANC)’s policy victories under Zuma’s leadership. Knowing that tobacco disproportionately affected certain racial and minority groups, Zuma made tobacco control a top priority. With the support of the President, local tobacco experts, and anti-tobacco advocates, Zuma worked hard to break previous connections between the government and the tobacco industry and to reduce smoking. The case ends in 1996 when smoking prevalence had declined to 32% from 34% in 1995, but South Africa still had one of the highest levels in the developing world. As the ANC was preparing to enact the new Constitution that reinforced health promotion, Zuma had to determine what her next move would be for tobacco control and how she would prioritize it with the other health needs of the country.
Teaching Note available through Harvard Business Publishing.

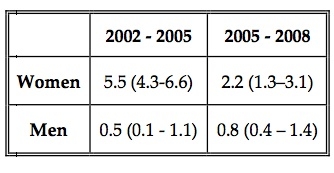
Tobacco Control as Health Promotion. Source: Reddy, SP and Swart D. Unraveling Health Promotion: A Framework for Action: Tobacco Control. MRC: 1998. (Exhibit 8 in "Tobacco Control in South Africa" case.)
Learning Objectives: To understand the political and economic forces that impact tobacco control legislation in a country undergoing an epidemiological shift, the role of research and data, and the value of health communication, chronic disease prevention, and advocacy in health care delivery.
Supporting Content: This case has a supplementary summary of history and next steps, titled Tobacco Control in South Africa: Next Steps.
Keywords: Chronic disease prevention, advocacy, health policy, tobacco control

















{kind=link}